Health Connection - March 2023

Women and Heart Disease: Knowledge to Take to Heart
By Ines Sherifi, MD, MSc and Rebecca Pease, RN

What do food poisoning, panic attacks, acid reflux, asthma, muscle strain, fatigue, and flu have in common? In women, they may be an indication of a heart attack. As a result, women may shrug off their symptoms when having a “silent heart attack,” also known as silent ischemia. A silent heart attack may have confusing or unrecognized symptoms, minimal symptoms, or even no symptoms at all. A woman may not even realize she has had a heart attack until months later, when her physician diagnoses scarring and damage to the heart, putting her at risk for additional heart attacks or heart failure.
Heart disease is the leading killer of U.S. women, surpassing all cancers combined. This translates to one in three female deaths, or approximately one woman every minute. There are several reasons for these somber statistics. Women’s heart attack symptoms are often more subtle, and women may not even realize they are having a heart attack.
Women’s Heart Attack Symptoms
It is important to understand the difference between a heart attack and cardiac arrest. The Hollywood heart attack, in which an actor dramatically clutches his chest and hits the ground, is a cardiac arrest. This is when the heart stops pumping blood, and breathing is interrupted. A heart attack is caused by a blockage of the coronary arteries. Left untreated, the heart muscle is deprived of oxygen and starts to die. Heart attacks generally manifest through chest pain and tightness in men. Women’s symptoms are more subtle. They may include:
- Lightheadedness
- Shortness of breath
- Jaw pain
- Neck pain
- Stomach pain
- Pain in one or both arms
- Nausea and vomiting
- A cold sweat
(While the above symptoms are more common in women, they can sometimes occur in men as well and should not be ignored, regardless of a person’s sex.)
Denial Can Be Deadly
The median time it takes women to see a doctor after experiencing a heart attack is 54 hours, vs. 16 hours for men. A woman may minimize her symptoms or rationalize them away as fatigue, heartburn, or muscle pain. Younger women who exercise, have healthy eating habits, and are not overweight may not even consider that they could have had a heart attack. Sadly, ignoring heart attack symptoms can have dire consequences. Recent studies found that, compared to men, women have a 20% increased risk of developing heart failure or dying within five years after their first severe heart attack. Post-heart attack, women’s rates of heart failure and stroke are also higher. Within five years, 47% of women who have suffered a heart attack will die, develop heart failure, or suffer from a stroke, compared to 36% of men.
Know Your Risk Factors
When it comes to women’s heart disease, lack of awareness of risk factors is a risk factor in itself. It’s critical to assess and understand your risk.
Some risk factors apply to both sexes:
- Family history of heart disease
- High blood pressure
- Elevated levels of LDL, or “bad” cholesterol
- Diabetes
- Obesity
- A sedentary lifestyle
- Tobacco use, including exposure to second hand smoke
- Excessive alcohol use (more than one drink a day for women, 2 for men)
- A diet high in saturated fats, trans fat, and cholesterol
- Depression and stress
- Age. Heart attack can occur at any age, but the risk increases over time, starting at age 45 for men and 50 for women
In addition, some risk factors are specific to women, including:
- Polycystic ovarian syndrome (PCOS), a hormonal disorder that can cause hair loss, menstrual irregularities, obesity, high blood pressure, and metabolic syndrome.
- Peripartum cardiomyopathy, a weakness of the heart muscle which can occur between the final month of pregnancy and five months after delivery.
- Takotsubo cardiomyopathy, also known as broken-heart syndrome, a weakening of the left ventricle that usually occurs during severe emotional or physical stress, such as the death of a loved one.
- Preeclampsia, a sudden, dangerous rise in blood pressure in pregnant women whose blood pressure had previously been normal.
- Gestational diabetes
- Early age of a woman’s first period
- Early menopause
- A history of miscarriage and/or preterm birth
- Premenstrual syndrome (PMS)
MarinHealth’s Women's Heart Program
MarinHealth launched a new Women’s Heart Health Program offering preventive strategies, screening, education, nutrition coaching, and cardiac rehabilitation. The program provides a multidisciplinary care approach that promotes collaboration between primary care physicians, OB/GYNs, endocrinologists, maternal-fetal medicine specialists, and cardiologists to establish diagnostic pathways, treatment, and ongoing monitoring for women at risk for heart disease.
The MarinHealth Women’s Heart Health Program is made possible in part through the generosity of the Haynes family. Their dedication and generosity have enhanced the leading-edge cardiovascular care available at MarinHealth's Haynes Cardiovascular Institute.
Patients at risk of heart disease can be referred to the Women’s Heart Program by their primary or specialty care providers and can self-refer by calling 1-628-336-5395. For more information about the Women’s Heart Health Program, visit https://www.mymarinhealth.org/womensheart.
Dr. Ines Sherifi is a board-certified cardiologist, cardiovascular imaging specialist, and medical director of MarinHealth's Women’s Heart Health Program. Rebecca Pease, RN, is the patient navigator for MarinHealth's Women’s Heart Health Program at MarinHealth Cardiovascular Medicine | A UCSF Health Clinic.
Scan Yourself for Skin Cancer – Here’s How
By Matthew M. Koehler, DO, FAAD, FAOCD

Skin cancer is most curable when diagnosed early. That’s why most dermatologists recommend performing this health routine regularly, ideally once a month.
Checking Your Skin
Set the stage
You may find it convenient to do the scan in your bathroom, before taking a bath or shower. Remove your clothing and perform the skin scan in front of a full-length mirror in a well-lit room. Have a hand-held mirror handy to look at hard-to-see areas in the back of your body.
Get a baseline
The first time you perform your skin check, closely observe all moles, freckles, and other marks on your skin, so you’ll know what’s normal for you and notice changes over time. Your cell phone can be a useful tool for taking visual notes. Be sure to see a doctor if you find anything concerning, even if it’s your first scan.
Examine yourself in the mirror
Stand in front of the mirror to check your face, ears, neck, chest, and belly. Don’t overlook hidden areas like your underarms, between your fingers and toes, your palms, and under your fingernails. If you are a woman, lift your breasts and look underneath. Be sure to check both sides of your arms and hands.
Have a seat
Examine the front of your thighs, shins, tops of the feet, in between your toes, and under your toenails.
Use the hand mirror for hard-to-see areas
Look at the bottom of your feet, calves, and the back of your thighs—first checking one leg and then the other. If you're comfortable doing so, ask a spouse, friend, or family member to help you check your lower and upper back, and the back of your neck and ears. If you're checking those areas solo, do your best to position the hand mirror so you can see them in the wall mirror. Use a comb or hair dryer to part your hair so that you can check your scalp. Don’t forget to examine your buttocks and genital area.
What if You Find a Suspicious Spot?
If you notice anything concerning, see your primary care physician or make an appointment with a dermatologist. If he or she can’t see you right away, take close-up pictures of the area so the doctor can note any changes when you come in. If the doctor suspects skin cancer, they will order a skin biopsy. A sample of the affected area will be removed for examination under a microscope.
Know Your Risk
Regardless of skin color, anyone can get skin cancer, even if their skin doesn’t typically sunburn. Regular skin checks are especially important if you have the following risk factors:
- Skin that burns, reddens, or freckles easily
- Light skin color
- Blond or red hair
- A large number of moles
- Personal history of skin cancer
- Family history of skin cancer
- Older age
- A history of sunburns, indoor tanning, and spending a lot of time outdoors
- Being over the age of 50, although skin cancer can, and does, occur in younger people
What to Look for
Skin cancer develops primarily on areas of the body that get a lot of sun exposure, including the scalp, face, lips, ears, neck, chest, arms, hands, and legs. However, lesions can also develop on less sun-exposed areas such as your palms, the soles of your feet and even under your nails, so don’t ignore skin changes anywhere on your body. These are the three most common forms of skin cancer:
- Basal cell carcinoma, which usually occurs on sun-exposed areas of the body such as the face, ears, and hands, and may appear as a pearly or waxy bump or a flat, flesh-colored, or brown lesion
- Squamous cell carcinoma generally occurs on sun-exposed areas of the body and may appear as a firm, red nodule, or a flat lesion with a crusty surface
- Melanoma is fast-growing, dangerous, and potentially deadly and can develop anywhere on the body, including in areas that are not exposed to the sun such as the mucous membranes of the mouth, nose, vagina, or anus
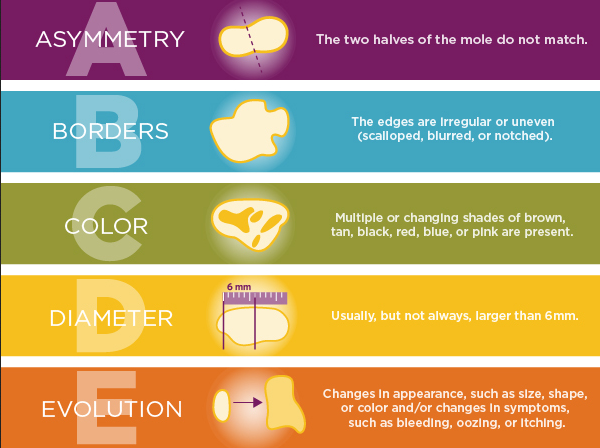
The ABCDEs of Melanoma
Here’s an easy way to remember the tell-tale signs of a possible melanoma:
MarinHealth Dermatology | A UCSF Health Clinic is a specialty practice specializing in medical, surgical, cosmetic, and pediatric dermatology. The newly affiliated practice includes seven board-certified dermatologists providing the highest level of personalized care in the diagnosis and treatment of skin cancers and the full spectrum of dermatologic conditions. Find a MarinHealth dermatologist near you.
Matthew M. Koehler, DO, is a board-certified dermatologist at MarinHealth Dermatology | A UCSF Health Clinic.
Who Knew? 10 Tips for Breastfeeding Moms
By Rachel L. Yang, MD, CLC, IBCLC

As a certified lactation counselor and international board-certified lactation consultant, Dr. Rachel Yang knows first-hand what nursing mothers ask about or wish they had known. Dr. Yang is a member of the Academy of Breastfeeding Medicine and the Institute for the Advancement of Breastfeeding & Lactation Education. She started the first breastfeeding medicine clinic in the Bay Area at MarinHealth, where she also works as a breast surgical oncologist. Dr. Yang helped us put together this list of useful and sometimes surprising information for nursing moms. Dr. Yang is currently breastfeeding her two young children.
Breastfeeding is a natural, age-old activity that centers around just two people: a mother and her baby. But there’s a lot of information – and misinformation – swirling around that loving duo. Grandmothers, friends, social media influencers, manufacturers hawking everything from pumps to massaging devices... it seems like everyone has different advice.
- Oops! Don’t forget to take these to the hospital.
Some lists include a nightgown, toiletries, lavender oil, or soothing music to give birth by, but they often omit nursing needs. I recommend packing a hands-free pumping bra, nipple balm, hydrogel pads, and wool or bamboo nipple pads. - Timing your baby's feedings is a waste of time.
After your infant has regained birth weight, let them set the timing for feeds. Once you and the baby have found your rhythm and breastfeeding is going smoothly, baby will stop feeding when satiated. Some babies only nurse from one breast at a time. I really encourage moms not to spend time looking at numbers of minutes on each breast. Instead, look at if the baby is gaining weight: Are they sucking and swallowing? Are they relaxed at the breast when they finish feeding? - Worrying about what’s “normal” is normal.
One thing that’s very common for first-time moms is worrying. Is my baby eating enough? Is she gaining enough weight? Is he pooping or peeing enough? Remember, those multi-tasking moms who make nursing look easy were once newbies themselves, with many of the concerns you’re dealing with today. For an overview of “normal,” the below chart is a good indicator of what to expect in those special first weeks.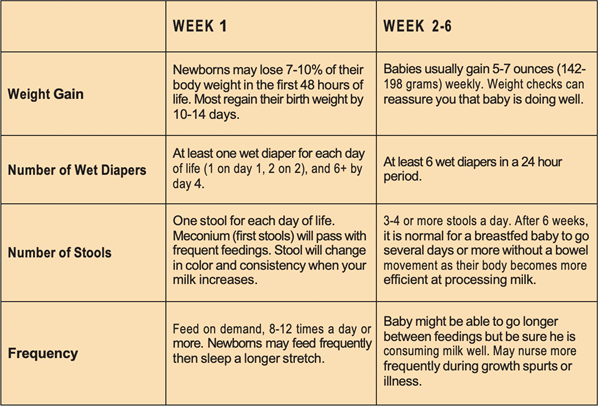
- Bad advice makes engorgement worse.
While removing small amounts of milk for comfort is safe, pumping or using a Haaka to remove milk when engorged before or after breastfeeding will only stimulate them to make more milk and worsen the engorgement. Sometimes, women with one “overactive” breast are advised to pump or continually feed the baby. Expressing more than the baby demands will trigger the body to make more milk than necessary, worsening engorgement. If you have ample milk production, feed the baby off the less full breast first. This allows the overproducing breast to remain full and gradually lessen production while encouraging the other breast to produce more milk. - To burp or not to burp?
If your mom keeps suggesting you burp the baby, she probably bottle-fed her children, or followed some old-school advice. The truth is, babies who nurse do not need to be burped like formula-fed babies. Burping often overstimulates a content baby and can create the false impression that he wants another feeding. If a baby is happy and asleep at the breast following a feed, there is no reason to burp. The one exception to this is a baby with GERD, or painful reflux, who is crying after a feed and feels relief with burping. - Nipple thrush is not a thing.
Oral thrush is uncommon in full-term breast-fed babies, but it can occur. This oral yeast infection causes white patches in and on baby’s mouth and gums. However, thrush is often mis-diagnosed in babies, as it can look similar to “milk tongue." Yeast is not transmissible to mother, and thus an infant with oral thrush is not a reason to treat mom. Also, there is no evidence to support yeast as a cause for nipple pain. While some doctors may prescribe antifungal creams for the mother, new research indicates that thrush does not occur on the nipples. Antifungals are unnecessary and may increase irritation or even cause an allergic reaction. - Nipple care no-no’s: Lay off the lanolin.
Nipple pain and wounds are common in those early postpartum days and caring for your nipples is essential. Unfortunately, many women are given bad advice. Make sure you DO NOT:
• “Dry out” nipples with saline soaks. This causes cracking from dry skin and makes pain worse.
• Use lanolin. 6-10% of women who use lanolin have an allergic reaction, which can derail your attempts to breastfeed.
I recommend applying an organic, lanolin-free nipple balm and then covering your nipples in a hydrogel “soothie” pad, which you can remove for nursing. Polymem or mepilex covers are another possibility, though they should not be used with nipple balm because they are more absorbent and less moisturizing than hydrogel combined with a balm. - No, your nipples are not weird.
Body positivity has come a long way, but women still worry about the shape of their nipples, especially when they are feeding a tiny human. Nipple shape, size, coloring, and positioning on the breast varies greatly from one woman to the next. There’s no perfect nipple shape. Even most inverted or flat nipples can be pulled out by the baby’s mouth. Nipple pain may be related to position, or high or low milk production. If the pain continues, reach out for help. - About that “perfect latch."
Of course, a good latch is essential, but there’s no such thing as a textbook latch. Moms are often focused on achieving the perfect latch; however, no comfortable latch can be achieved without the right position. If you notice that a portion of your areola is outside the baby’s mouth and the baby is swallowing contentedly and growing well, don’t worry. Women have different-sized areolae and different-sized babies. There are many babies who breastfeed and gain weight, even if their latch doesn’t look "perfect." - Treating “plugs” or “clogs”: anti-inflammatories and avoiding massage.
Evidence does not support the presence of true “plugs” or “clogs” in lactating milk ducts. These painful lumps are balls of inflammation in the breast tissue, usually caused by oversupply or dysbiosis. Treat these episodes with ice and ibuprofen. Avoid massaging the breast, as this can cause bruising and tissue damage and won’t alleviate mastitis. Pumping can increase inflammation and make the problem worse, so avoid this if you are able to exclusively feed at the breast. With direct breastfeed, baby’s saliva provides healthy bacteria and moves retrograde up the ducts of your breast to make a healthy microbiome. If pumping is needed, a probiotic can be used to improve the microbiome. Do not increase pumping or feeding to try to “empty the breast," as this only increases inflammation and milk production behind the inflamed area. When inflammation progresses to mastitis (red skin or fever >101.5), contact your provider; however, often antibiotics can be avoided using the techniques mentioned above.
To learn more, please check out my recent Interactive breastfeeding seminar with the Southern Marin Mothers' Group, streaming on the MarinHealth YouTube channel.
Urgent Matters: Should You Call Your Doctor, Visit Urgent Care, or Call 911?
When retired nurse Josephine moved to San Anselmo, she didn’t have time to establish a new primary care provider or wait for an appointment for her persistent throat pain. “After getting sick traveling in France, the pain was affecting my larynx, and my voice was cracking,” she said. When she called to make an appointment with a new provider, the MarinHealth Care Team suggested she might want to visit the MarinHealth Urgent Care | A UCSF Health Clinic in San Rafael if she felt her situation couldn’t wait.
"I’m so grateful the person I talked to suggested I go to urgent care,” said Josephine. “I saw Dr. John Clothier. He was empathetic and treated me with compassion. For the first time in recent years, it was the most comprehensive doctor’s visit I have had. He took time to listen to my health concerns in addition to my throat pain. He asked about my state of mind, and addressed my chronic sleep deprivation. He went beyond the ailment I was there for. Dr. Clothier was exactly the kind of doctor I was looking for, and I’m grateful he took the time to treat me as a person."
Josephine’s story showcases the choices patients have when they’re not feeling well and are considering the best way to move forward.
Emergency Situations
The Emergency Department at MarinHealth Medical Center offers comprehensive services, including life-saving care for major injuries, emergency spine and brain surgery, and award-winning care for heart attack and stroke. MarinHealth Medical Center is designated as a Level III Trauma Center, with a complete team available 24/7, including board-certified emergency physicians and other specialists, nurse practitioners, physician assistants, emergency technicians, and support staff.
Get the Help You Need, When You Need It
Urgent care is the perfect solution when your regular doctor isn’t available or you need fast treatment for an injury or illness that isn’t serious enough for the Emergency Department. From sprained ankles to earaches and allergy attacks, MarinHealth Urgent Care provides quick and convenient care to help you get back on your feet again.
MarinHealth Urgent Care Clinic is the perfect solution:
- When you need care outside of regular office hours
- When your doctor can’t fit you in soon enough
- When you need services your doctor doesn’t provide, such as stitches
Emergency Care vs Urgent Care vs 911
If you are unsure about the severity of your condition, see the chart below to help you decide where to go. If you are experiencing a medical emergency, please call 911, or visit your closest emergency room.
| Symptom | Urgent Care | Emergency | 911/Ambulance |
|---|---|---|---|
| Minor fractures, sprains, strains (no casting) | X | ||
| Head injuries | X | ||
| Allergies & asthma | X | ||
| Cold, flu, earache, headache, or sore throat | X | ||
| Upset stomach, diarrhea | X | ||
| Urinary tract infections | X | ||
| Fever under 105°F | X | ||
| Fever over 105°F | X | ||
| Cuts, rashes, or burns | X | ||
| Bleeding that won’t stop | X | ||
| Bad or worsening medication reaction, overdose or poisoning | X | ||
| Worsening reaction to an insect bite | X | ||
| Foreign body removal | X | ||
Possible heart attack*
| X | ||
Potential stroke
| X |
Appointments
You can schedule a same-day or next-day appointment at our Urgent Care Clinic online or by calling our office: 1-415-925-8865.
For Pediatric Patients
We offer after-hours care specifically for children — provided by pediatricians — at our Pediatric After-Hours Care Clinic in Larkspur. Open evenings and weekends, this location delivers specialized care for young patients, but we can also treat children three months of age and older at MarinHealth Urgent Care.

